Rehabilitation can be defined in many ways, but an approach used by the British Society of Rehabilitation Medicine describes rehabilitation in terms of both a concept and a service as follows:
Conceptual definition: A process of active change by which a person who has become disabled acquires the knowledge and skills needed for optimal physical, psychological and social function.
Service definition: The use of all means to minimise the impact of disabling conditions and to assist disabled people to achieve their desired level of autonomy and participation in society.
These terms can be usefully applied to people who have experienced major trauma. In addition, it needs to be acknowledged that severe injury of an individual affects a wider pool of people both directly and indirectly, and the needs of families and carers should also be addressed during the rehabilitation process.
A person sustaining a major trauma will have a multi-disciplinary team (MDT) involved in their rehabilitation pathway. The major trauma rehabilitation pathway means that rehabilitation commences at the earliest point after admission through the emergency department (ED), with a formal assessment resulting in a Rehabilitation Prescription within two working days of resuscitation and stabilisation. Major trauma rehabilitation pathway
Major trauma rehabilitation pathway
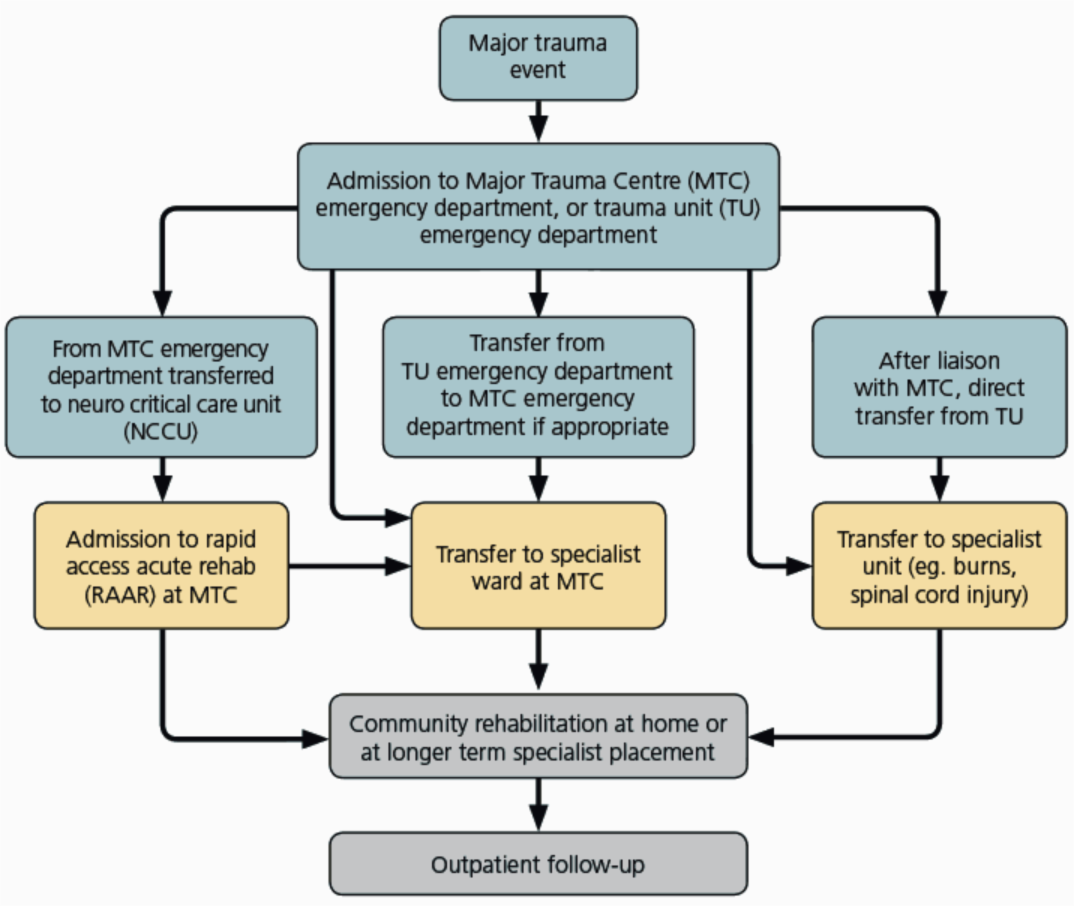
The Trauma Network will be following patients through the first year of their recovery. This will cover different stages in their rehabilitation pathway as outlined below. Support will be offered to families and carers throughout the pathway.
Acute rehabilitation
This stage is when the person is being treated in the MTC or other specialist unit, with the emphasis being on managing the original injuries and reducing the impact and likelihood of secondary complications. From a rehabilitation perspective, this would be described as focusing on impairment and secondary complications (pathology), eg. pressure sores, chest infection, malnutrition, contractures etc. The two working days rehabilitation prescription describes the domains addressed in detail.
Post-acute rehabilitation
This stage describes the period when patients are more medically and surgically stable (ie. out of the critical care/HDU settings) and well enough to actively participate in a rehabilitation programme. Post-acute rehabilitation primarily focuses on regaining mobility and independence in self-care with the aim of enabling the person to manage safely at home. Thus the interventions are aimed at reducing disability through promoting activity and independence. For severely injured individuals, this phase may last many months.
For patients unable to actively participate (those with disorders of consciousness or severe behavioural/cognitive disorder) in this phase, a rehabilitation programme is constructed around the patient, in their best interests.
Community rehabilitation
This final phase of rehabilitation is often the most prolonged and is essential to the optimisation of a person’s recovery. The emphasis is on more extended activities of daily living, social integration and return to work or education. Psychological adjustment to the injuries by the person and the impact of carer stress often come to the fore and need addressing. A focus on improving participation and enhancing quality of life is undertaken.
All these phases will be monitored by the trauma rehabilitation co-ordinator. Outcome measures one year following the trauma will be collected and audited.
References
National Service Framework for long-term conditions, Department of Health, 2005
Royal College of Physicians, Medical rehabilitation in 2011 and beyond, Report of a working party. London: RCP (2010)
British Society of Rehabilitation Medicine, Vocational assessment and rehabilitation for People with Long-Term Neurological Conditions: Recommendations for best practice, BSRM (2010)
World Health Organisation International Classification of Functioning, Disability and Health (ICF), WHO, 2001