Traumatic injuries of the cervical spine are uncommon in children. They are primarily seen in 1 to 2 percent of children who sustain blunt trauma. However, it is essential to assume cervical spine injury in every injured child until examination and / or radiological investigation prove otherwise. Injury may involve bones, ligaments, blood vessels, and/or the spinal cord, and must be rapidly recognised and treated to avoid permanent disability or death. Patients with suspected or possible cervical spine injury must have their cervical spine properly immobilised until formal assessment occurs. If the patient doesn’t need intensive care, the responsibility of cervical spine clearance lies with the trauma team leader.
Indications for C-spine immobilisation:
- All children with altered level of consciousness
- Patients in whom the mechanism of the injury could have resulted in injury to the spine
- All patients with signs and symptoms consistent with spinal cord injury:
- history of transient paraesthesia, dysaesthesia, shooting pains or subjective extremity paralysis
- complaints of neck pain or discomfort, or presence of muscle spasm
- limited range of motion or tenderness over the spin
- presence of sensory-motor deficits.
Full and correct immobilisation includes all of the following:
- Neutral position on a firm surface. If child is more than 3 years of age, use hard collar reinforced by blocks or sandbags with tape.
- If child is less than 3 years of age, blocks or sandbags and tape.
- Where above not available, manual in-line immobilisation must be used.
Note: hard collar must be the correct size for the patient and soft collars are not acceptable.
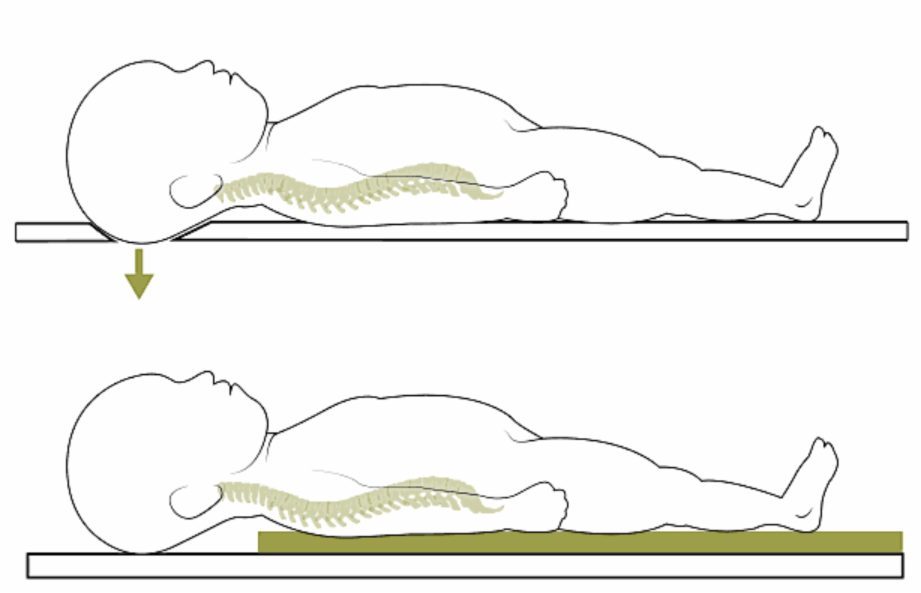
In children under 2 years of age, who have larger heads, the following should be done:
occipital recess or thoracic and lumbar support (as shown below) sandbags/tapes and hard collar for young children.
Constant reassurance is required to help keep the child still and reduce their anxiety levels. If the child is anxious or unco-operative and a thorough examination is not possible, try and maintain in line C-spine immobilisation with or without a collar.
Imaging for cervical spine injuries: NICE Guideline 56 – Investigation in the ED
- Children aged 10 years or more can be treated as adults for the purposes of cervical spine imaging.
- Children under 10 years should receive anterior/posterior and lateral plain films without an anterior/posterior peg view.
- Children under 10 have increased risk from irradiation, so restrict CT imaging of
cervical spine to children with indicators of more serious injury, in circumstances
such as:
- severe head injury (GCS ≤ 8)
- strong suspicion of injury despite normal plain films
- plain films are inadequate.
As a minimum CT imaging should cover any areas of concern or uncertainty on plain film or clinical grounds.
Selection of children (age 10+) for imaging of the cervical spine:
NICE Guideline 176 – Investigation in the ED
Are any of the following present?
Check both lists
| Patient cannot actively rotate neck to 45° to left and right, check only if safe to do so1 | GCS < 13 on initial assessment | |||||||
| Not safe to assess range of movement in the neck | Has been intubated | |||||||
| Neck pain or midline tenderness plus dangerous mechanism of injury2 | Plain film series technically inadequate (for example, desired view unavailable), suspicious or definitely abnormal | |||||||
| Definitive diagnosis of cervical spine injury required urgently (for example prior to surgery) | Continued clinical suspicion of injury despite normal X-ray | |||||||
| Patient is being scanned for multi-region trauma | ||||||||
| Yes |
No |
No |
Yes |
|||||
| Request three view radiographs immediately | No imaging required now | Request CT scan immediately | ||||||
- Safe assessment can be carried out if patient: was involved in a simple rear-end motor vehicle collision; is comfortable in a sitting position in the emergency department, has been ambulatory at any time since injury and there is no midline cervical spine tenderness, or if the patient presents with delayed onset of neck pain.
- Dangerous mechanism of injury: fall from > 1 m or 5 stairs; axial load to head – for example, diving; high-speed motor vehicle collision, rollover motor accident, ejection from a motor vehicle, accident involving motorized recreational vehicles, bicycle collision.