Major incidents involving multiple patients with serious injuries
Many major incidents for the health services involve trauma. There are well
rehearsed plans in place in all organisations to manage these incidents, and
the Trauma Network does not wish to replace these but seeks to optimise the
care of all severely injured patients.
The Trauma Network and its partners have agreed the following principles
regarding major incidents involving multiple patients with serious injuries.
Pre-hospital
- A good METHANE report is essential
- In a major incident, pre-hospital responders should not use the trauma triage tool – the existing system of major incident triage should be used in order to avoid confusion
- Assume that patients triaged as P1 are trauma triage tool positive patients
- Assume that patients triaged as P2 and P3 are trauma triage tool negative patients
- The aim should be to get P1 patients to a major trauma centre (MTC)
- this will involve effective use of transport resources including SAR or a helicopter with/without a medical team
- P1 patients with uncontrollable airway, breathing or circulation problems should be taken to the nearest trauma receiving hospital (MTC or TU)
- If the MTC is unable to manage the number of patients being transferred to it, the Trauma Network Co-ordination Service (NCS) and Ambulance Trust will co-ordinate a divert arrangement
- While it is recognised that P2 patients may satisfy criteria for transfer to the MTC from the scene, it is important that the MTC is not overwhelmed as further patients may require transfer. The receiving hospital for these patients is therefore likely to be a trauma unit (TU) able to do initial assessment, treatment and stabilisation
- P3 patients may be taken to an appropriate facility. This may include a TU, a local emergency hospital (LEH) or other approved local provider. However, it is important that it is appreciated that triage category may change as injuries manifest or patients receive treatment
Acute hospitals
- Major incident plans remain essentially unchanged
- The NCS is available for both clinical advice, transfer support and must
importantly still be able to track all trauma patients in the region
- the addition of NCS telephone number to Trust Medical Silver Command (or equivalent) and ED Bronze Commander action cards and information sheets may be useful
- If the incident is outside the east of England (EoE) and patients are received within an EoE TU or MTC, the NCS should be informed and can support as normal.
- Patients transported initially to a TU may require further definitive treatment at an alternative tertiary centre. This should be co-ordinated through the NCS.
- Transfer of patients to the MTC or other specialist unit from a TU may take place over a longer period of time than for a single seriously injured patient once initial assessment and damage control treatment is done. Timing will depend on the capability of the MTC and available transport options and a TU should plan for holding patients for longer where there are multiple casualties
Network Co-ordination Service (NCS)
- NCS should remain the focus for co-ordination of trauma patient care – particularly needs to know where trauma patients (all P1 and those P2 that transpire to have major trauma) are, and can support transfer
- NCS will link closely with the MTC, EEAST and regional bodies to support trauma patients
Recovery phase
- Standard principles apply for repatriation and a TU should expect to receive patients back within 48 hours of notification as usual in order to maintain flow within the MTC. If there has been cross-boundary mutual aid, patients may need to be repatriated from MTCs in other Regions
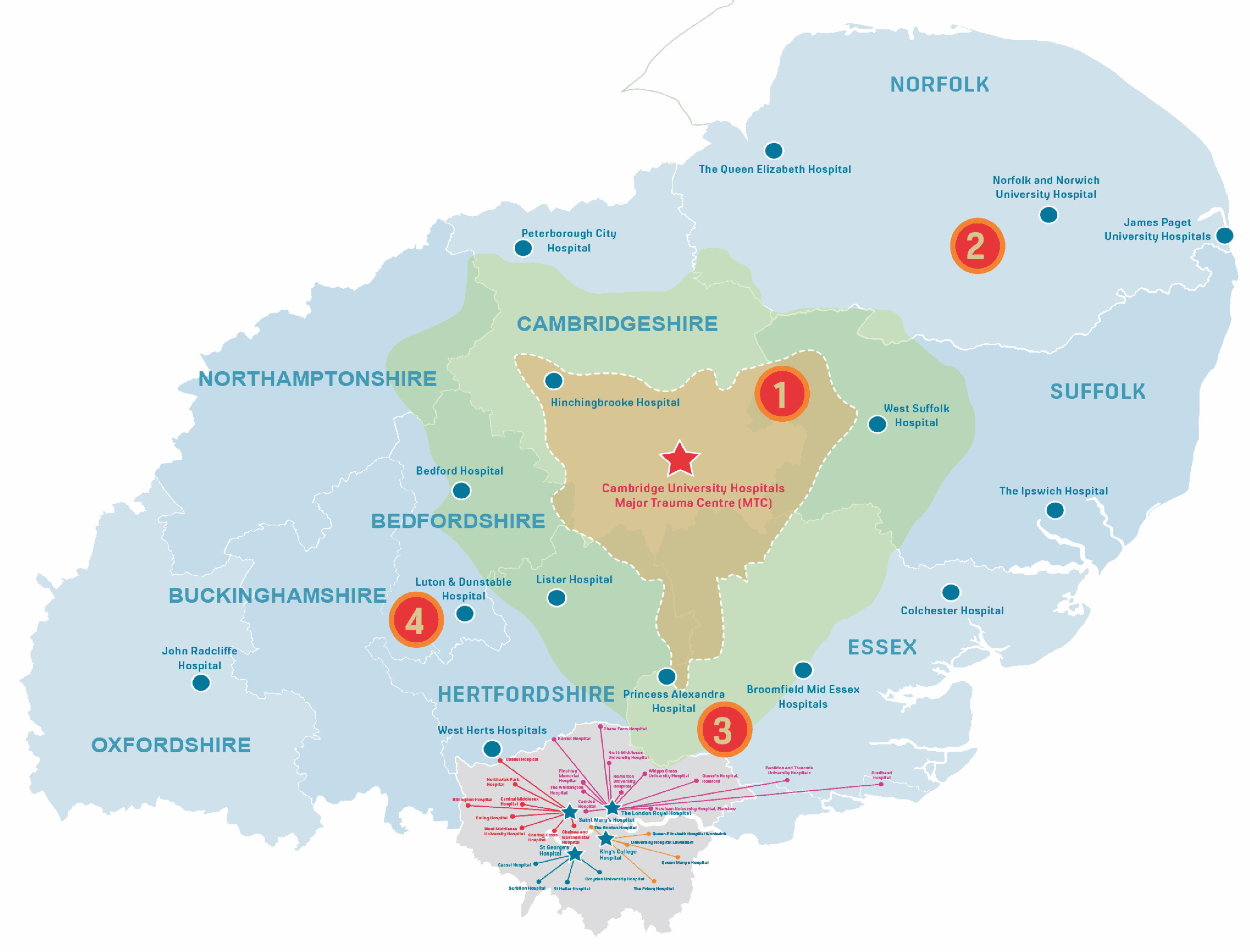
| Scenario | 1 |
Tuesday, 10am
Multiple vehicle road traffic incident
| P1 | P2 | P3 |
| 20 | 20 | 20 |
- MAJOR INCIDENT declared by first pre-hospital responders on-scene – METHANE report given
- Ambulance service major incident plan activated and followed
- P1 patients triaged preferentially to the MTC at Cambridge University Hospitals
- P2 patients triaged to West Suffolk Hospital
- NCS tracks patients and can give advice on clinical care and transfers from scene or TU
| Scenario | 2 |
Tuesday, 2am
Multiple vehicle road traffic incident
| P1 | P2 | P3 |
| 20 | 20 | 20 |
- MAJOR INCIDENT declared by first pre-hospital responders on-scene – METHANE report given
- Ambulance service major incident plan activated and followed
- P1 patients triaged preferentially to the MTC at Cambridge University Hospitals
This may involve using search and rescue capabilities - P2 patients triaged to Norfolk and Norwich University Hospital and James Paget University Hospital
- NCS tracks patients and can give advice on clinical care and transfers from scene or TU
| Scenario | 3 |
Wednesday, 3pm
Multiple vehicle road traffic incident
| P1 | P2 | P3 |
| 20 | 20 | 20 |
- MAJOR INCIDENT declared by first pre-hospital responders on-scene – METHANE report given
- Ambulance service major incident plan activated and followed
- P1 patients triaged preferentially to the MTC at Royal London Hospital
- P2 patients triaged to Mid-Essex Hospital and Princess Alexandra Hospital
- NCS tracks patients and can give advice on clinical care and transfers from scene, MTC or TU
| Scenario | 4 |
Wednesday, 3pm
Aeroplane crash
| P1 | P2 | P3 |
| 40 | 20 | 20 |
- MAJOR INCIDENT declared by first pre-hospital responders on-scene – METHANE report given
- Ambulance service major incident plan activated and followed
- P1 patients triaged preferentially to the MTC at Cambridge University Hospitals. NCS communicates with other Trauma Networks and EEAST to co-ordinate P1 patients also going to MTCs at Coventry / St Mary’s / Oxford
- P2 patients triaged to Luton & Dunstable Hospital
- NCS tracks patients and can give advice on clinical care and transfers from scene, MTC or TU